Written In Ink
Cancer and the Choice to Draw a Line
The Margins
I was being admitted into UCLA Cancer Center in Santa Monica, California, after a two-and-a-half-hour ambulance ride. Newly diagnosed with an aggressive form of non-Hodgkin lymphoma that had already begun to overtake my body.
I was wheeled in through the back of the hospital, through the busy, overcrowded emergency room, down a long hallway, past a large, beautiful, open garden in the center of the hospital, into a wide elevator, and up to the fourth floor. Room 4212.
I'd been waiting over a week to be transferred there. It was one of the only two hospitals on the West Coast capable of handling my treatment and care.
If I didn't start treatment soon, my lungs would continue filling with fluid. One had already partially collapsed. Oxygen and steroids were the only things making breathing possible. My heart was under considerable stress as the tumor continued to grow in the center of my chest. Blood flow to my brain was being restricted as the tumor compressed the main vein, causing neurological issues. The headaches were unbearable. There was serious concern that the cancer would spread to my brain. If that happened, all bets were off.
The plan was to start an aggressive chemotherapy regimen called DA-EPOCH-R, along with chemotherapy injections into my spine. Radiation wasn't an option. Surgery wasnt an option. The treatment itself carried life-threatening risks and complications: tumor lysis syndrome, central nervous system issues, brain infections, neutropenia, sepsis, pneumonia, and cardiac and lung damage or failure. There was the risk of secondary cancers developing, and the reality that my body would not have enough white blood cells or be strong enough to fight the smallest infection.
As one Oncologist at the previous hospital put it when she walked into my room, glanced at my chart, and said in a strong foreign accent, “If you don't do this, you die,” before walking out. This was the road forward.
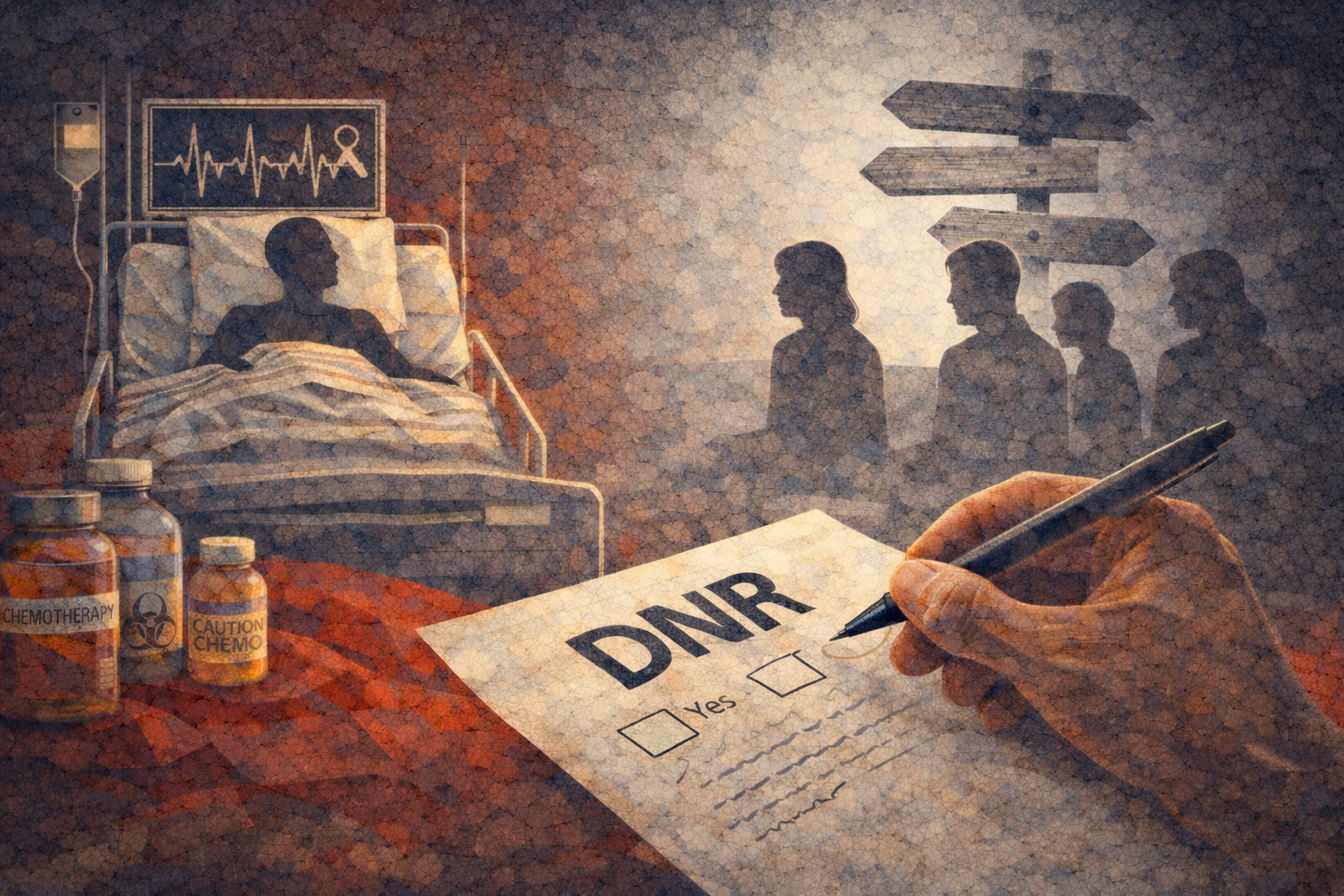
During the intake questionnaire with the lead nurse on my care team, I was asked whether I had a DNR order already in place.
A DNR? What was that?
The lead nurse nodded and said she would have someone come explain what it was and why it was important to have one going forward.
What’s A DNR?
When I think back on this memory, it frustrates me that I can remember exactly what this woman looked like, how she styled her hair, and what she wore, but I can't remember her name. In my mind, I squint at the memory, trying to make out her name tag, but it's blurred, the details are missing.
What I do remember is that she was a cheerful, agreeable older woman with short brown hair just past her ears, rosy cheeks, and a smile that never seemed to leave her face. She carried a black backpack and a thin white-and-blue folder. She introduced herself as one of the hospital’s patient social workers who helped educate terminally ill patients with end-of-life palliative care planning and DNRs.
“DNR stands for 'Do Not Resuscitate,” She told me.
It’s a legally binding form that outlines a patient's wishes in the event of complications requiring cardiopulmonary resuscitation (CPR) or other emergency life-saving measures. It ensures medical staff know exactly how far to intervene if something goes wrong.
At the time, I didn't realize how much of my understanding of life-saving care came from television and movies. The crash cart, CPR, dramatic recoveries, the heart monitor beeping as the patient comes back to life. I was a bit confused, almost in disbelief.
You mean to tell me some people choose against life-saving care!?
She explained to me that things were more complicated than that. Life-saving care comes with real risks and consequences. Things patients need to understand beforehand.
CPR, she explained, has only a 20 percent survival rate, significantly lower for older patients or those with complex medical conditions. The physical act of CPR, compressions to the chest, can often fracture ribs or the sternum. Those fractures can puncture lungs or cause internal bleeding. The risk of hypoxia during resuscitation means that the patient could be left with permanent neurological impairments. For patients with compromised immune systems, like cancer patients, these injuries can lead to severe infections and death.
She also explained that a patient might need to be put on a ventilator. Intubation, prolonged time on a breathing machine, and not using the throat muscles can damage the throat, vocal cords, and trachea. Some patients spend years in therapy learning how to speak or eat solid food again.
By the time she finished explaining each form of life-saving care, the odds, the complications, the risks, I began to understand that the DNR wasnt about refusing care.
It was about understanding the realities of life after. The realities and struggles that could exist, and choosing your own quality of life.

Defining My Limits
Cancer was forcing me to confront what survival might realistically look like, and how far I was willing to go to keep breathing.
It wasn’t a fair question, but the hospital needed to know how to treat me if something went wrong, and in my condition, the odds of that happening were real.
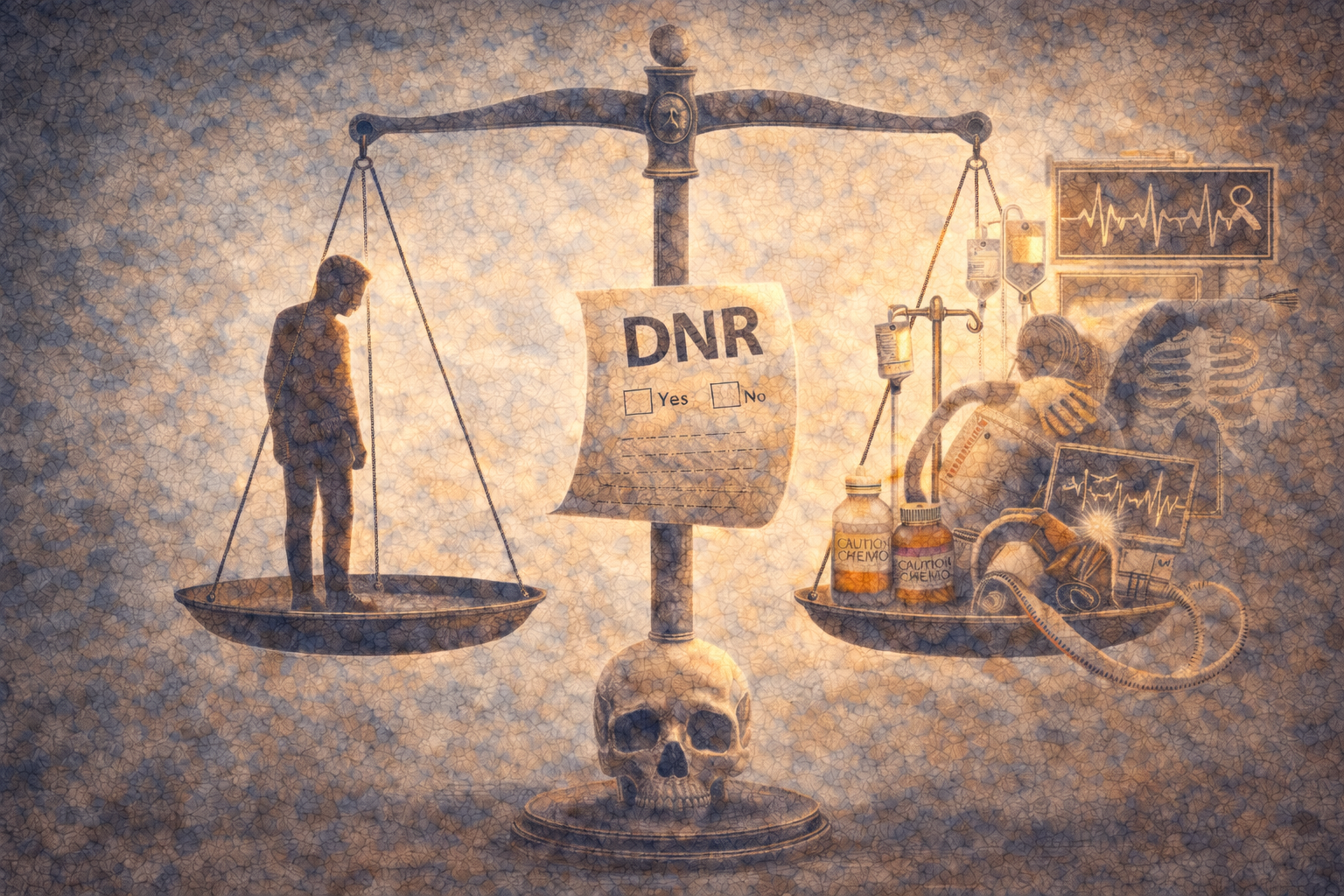
As I read through the paperwork and checked the boxes outlining my wishes, the question being asked was simple.
What level of suffering are you willing to endure for a chance at survival? And more importantly, what quality of life means to you when survival is uncertain.
Most people don't have to face these questions till much later in their life. Thinking about your own death isn't easy. It's imagining the worst scenario. From where I sat in that hospital bed, it wasn't too hard to imagine.
It scared me.
Living is the most selfish thing a person can do. It requires taking up space. It requires resources. It requires the sacrifice of others. But it's not a bad thing. Life is beautiful, and I wanted more.
More memories. More experiences. More smiles. More laughs. More love. More tasty food. More sunrises and sunsets. More passionate love-making. More time next to the people I love.
At first, my instinct was defensive. Signing the DNR felt like accepting defeat. I didn’t want to be remembered as someone who didn't fight for life. Who quit at the very end. Wanting to live felt synonymous with wanting every life-saving measure.
But as the conversation continued, I was forced to confront another reality. What was my body actually capable of handling? Would survival be practical? What would it cost my family, emotionally, physically, financially?
I don’t think there's a correct answer. Wanting to fight to the very end is valid. Wanting a peaceful exit without prolonged pain and suffering is also valid. Defining limits doesn't mean giving up.
I signed those papers.
The notary was scheduled and came later to make the form official and legal. The Social worker submitted the forms to the hospital and placed them into my file. I felt a sense of resolve after. I felt intentional, grounded. With so much uncertainty ahead of me, at least in this area, I knew how things would end.

Finding My Peace
When my parents later came to visit me, I gave them a copy of the DNR and told them these were my wishes if things took a turn for the worse. I told them we didn't need to talk about it right now. I wasnt looking for approval. I was communicating my choice.
Over the years of fighting this cancer and its complications, I've seen just how bad things can get. Ive lived in a body that no longer functions the way it should. Where pain was constant and progress uncertain. I’ve experienced days when hope felt unreachable. When my body and mind had reached their limits. I've cried from pain, and spent long stretches in silence when there were no tears left, only numbness.
I've also watched other cancer fighters in the rooms next to mine endure their own battles. Some are no longer here. What stays with me isnt just their absence, it’s the amount of pain they carried for so long before it ended.
Now, they’re at peace. And I wish peace for everyone in the end.
Facing the realities of end-of-life care doesn't mean you want to die. It means you're willing to be honest with yourself about what medicine can and can't do, and decide where the line is for you.
For me, it brought clarity. If things ever reached that point, my peace was already decided. Written in ink.

Written By Josh Parra
Cancer Survivor, Writer, Advocate